A systematic review of the factors affecting the provision of social support from co-workers during the return-to-work process

Introduction
Work, in the majority of cases, has been shown to have greater benefits to health and well-being than unemployment. Waddell and Burton (2006) found that for most people work provides resources necessary for economic well-being. Furthermore they reviewed strong evidence that work also allows individuals to meet their psychosocial needs for identity, self-esteem, and social status. Correspondingly, unemployment was found to be consistently associated with poor mental and physical health (Waddell and Burton 2006). Sickness absence is estimated to cost employers in the UK £9 billion per year and to cost the state £13 billion (Black and Frost 2011). Long term absence from work due to sickness can therefore be very costly both financially and in terms of health and wellbeing. It is important that efforts be made to increase the ease with which people are able to return-to-work (RTW) in a sustainable and timely manner.
The availability of social support from colleagues has consistently been found to have an effect on RTW success (e.g. Norlund 2013), and this is likely to be related to the benefits to well-being that result from feelings of belonging within a supportive work environment (Inman 2007). In the pursuit of improving current understanding, a body of research has begun to investigate the conditions under which social support is more, or less likely to be provided. A number of factors have emerged such as whether work accommodations entail extra work for co-workers, whether the returning worker’s claims of illness are trusted (Eakin et al 2003) and whether the illness suffered by the returning worker carries stigma (Brouwer et al 2010). Furthermore, Dunstan and MacEachen (2014) have developed a model of co-worker responses to work accommodations provided for an injured colleague. They suggest that factors such as attributes of the injured worker (e.g. gender, race, competence) and features of the injury affect social support behaviours via the co-worker’s judgement of the fairness of the work accommodations. This model presents a coherent and plausible account of the process however the studies which informed its creation did not specifically consider the RTW process but rather supported employment for a disabled employee. The following review of studies, which have considered factors affecting social support during the RTW process, allows further development and validation of this model.
The increasing number of qualitative studies investigating social support in the RTW process provided an opportunity to collate and synthesise these findings in order that a comprehensive and coherent understanding of the factors affecting social support could be reached. Once synthesised, the findings presented may allow RTW specialists, including occupational therapists, to better understand the optimal conditions for a successful return to work in order that they can best support returning workers.
The aim of this systematic review using meta-ethnography was therefore to investigate the factors influencing provision of social support by co-workers to a colleague returning after sickness absence.
Method
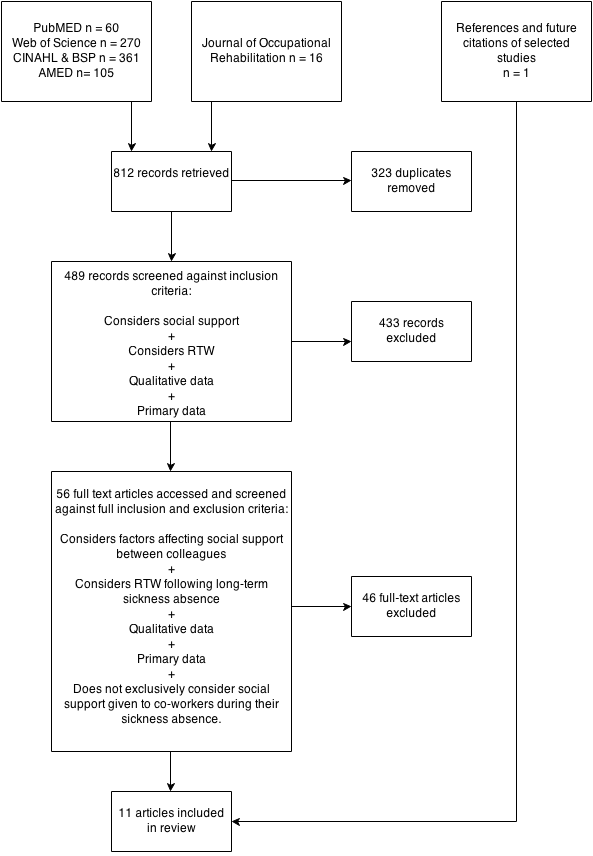
In January 2014 (08/01/14), several databases were searched for articles relating to the factors affecting social support given to colleagues returning from sickness absence. Databases searched included PubMED, Web of Science, CINAHL, Business Source Premier, and AMED. The search terms used were: co-worker OR colleague “return-to-work” OR “sickness absence” AND “social support”. Only articles published since 2000 were included to ensure study findings were relevant to today’s workplaces.
Following retrieval, records were screened using the inclusion and exclusion criteria as follows:
- Considers factors affecting social support
- Considers RTW following long term sickness absence
- Qualitative data
- Primary data
- Does not exclusively consider social support given during absence from work.
The Journal of Occupational Rehabilitation was also hand searched for further relevant articles as were the references and citations of selected studies. Studies published between January 2014 – November 2014 which cited the selected studies were further screened on 01/12/14. Fig. 1 (below) depicts the articles retrieved at each stage of the systematic search.
A data extraction form that included criteria from the CASP checklist for qualitative research (Critical Appraisal Skills Programme 2013) was used to record key findings and methodological details. Methodological quality ratings were then assigned to each study by comparing the results of the CASP checklist with Cesario et al’s qualitative levels of evidence (2002). Critical appraisal of study quality was performed in order to improve understanding of the methodological processes of the studies, and to ascertain how much confidence should be placed in the findings of certain studies. No studies were excluded as a result of this appraisal.
Data analysis
Relevant data from the selected studies were synthesised using meta-ethnography, as developed by Noblit and Hare (1988).
Meta-ethnography represents a means of synthesising qualitative studies in order that the end-product is not merely an aggregation of findings but a synergy that offers new understanding and prompts further research. Key concepts are identified within each study through a process of induction and these are compared and contrasted in order to generate novel interpretations. Meta-ethnography attempts to maintain the original terminologies used by participants and primary authors throughout the synthesis in order to improve the validity of the resulting synthesis. There are a series of phases that make up the meta-ethnography process.
Noblit and Hare (1988) describe the first three phases as involving selecting the studies for review and becoming familiar with them. Phase four involves the determination of relationships between each study. Key concepts are identified for each study and entered into a table through which the similarities and differences between studies begin to appear. In phase five the studies are translated into one another. This is done by attempting to locate each study’s unique concepts and metaphors within the other studies in order to identify similarities and differences between studies. Common concepts are categorized into themes.
The sixth phase concerns synthesizing translations: A decision is made about whether the concepts arising from each study can be described as relating to one another reciprocally, in a refutational sense, or as components of a line of argument. Reciprocally related concepts are those that are so similar they could encompass one another. Concepts related in a refutational sense are those that oppose each other. Finally, concepts that relate to one another in a Line of Argument are those that describe different aspects of a single phenomenon and combine to provide a fuller understanding of that phenomenon. The final phase involves expression of the synthesis, which in this case, will be in written form.
Statement of researcher’s interests
This research is underpinned by a constructivist epistemology, which Paterson et al (2001) claim is compatible with attempts to synthesise qualitative literature. In line with this epistemology, it is accepted that the interpretations made herein reflect the first author’s individual worldview and alternative interpretations are plausible. A reflexive diary and research supervision with the second author was maintained throughout the research process in order that any personal assumptions or expectations could be monitored.
Analysis
Sixteen articles met the inclusion criteria for this review. Of these articles, seven were assigned a good quality rating, and nine were assigned a medium quality rating using Cesario et al’s qualitative levels of evidence (2002).
Factors related to individual workplace actors
Characteristics of the returning worker
In several studies, the returning worker’s character or perceived character was influential to the provision of social support. A key attribute was the worker’s attitude; Participants in several studies spoke of social support that was dependent on the returning worker having the ‘right’ attitude which involved willingness to work hard towards making the return successful and being honest.
One participant in Dunstan and Maceachen’s study (2013) who worked in a military camp reported:
…as long as they [the returning worker] don’t have an attitude to give up or whatever, we kinda look after them as one of our own. (p.48)
Values of co-workers
In several studies, participants reported personal factors that encouraged them or others to provide social support, such as enjoying helping people or having a good pre-existing relationship with the returning worker. Furthermore participants in Sager and James’ study (2005) study discussed how having been through the RTW process was often a pre-requisite for social support:
… people don’t understand unless they experience it themselves. (p.133)
Influence of the supervisor
Four studies discussed the role of the supervisor in either facilitating or hindering the provision of social support among employees. The support behaviours they modelled were particularly influential. In a study conducted within the competitive electrical sector (Kosny et al 2012), managers were reported to have made attempts to prevent social support being given to returning workers, and one participant even reported workers had been rewarded for harassing a returning worker.
If a guy’s worked for a company and he’s really giving it to [the injured worker]…he made it so bad that this guy quit when he was injured, well the company is going to say…hey come on, I’ve got a job for you. (p.446)
The presence of the supervisor in RTW planning also appears very influential; participants in two studies reported feeling that without the guidance of a supervisor, misunderstandings and conflict were more likely to occur.
Factors related to the condition
History of illness
The returning worker’s illness history had an influence on provision of social support in several studies; the duration of a worker’s recovery and the number of previous absences led to reports of impatience on the co-workers’ part in several studies. Participants in Tjulin et al’s study (2011a) felt ‘drained of goodwill’ as time went on (p.1984).
Mental Health Problems
The existence of a mental health problem led to feelings of unease in several studies. Participants in Dunstan and Maceachen’s study (2013) reported feeling nervous of ‘provoking the workers’ mental condition’ (p.50) and therefore refrained from providing social support. A similar lack of knowledge about mental illness was reported to cause prejudice and discrimination in a separate study.
Another factor related to the returning worker’s condition that was reported as influential to the provision or withholding of social support was the visibility of their condition; several studies reported that a visible injury was more likely to be accepted and accommodated by co-workers than invisible conditions which led to doubt and distrust.
Lack of trust in the veracity of sickness absence claims
The validity of a condition was often called into question if it was not immediately visible and also if negative stereotypes were held about injured workers.
These stereotypes typically concerned ideas that the worker was irresponsible and had carelessly caused their injury, was lazy, or was trying to take the “easy way out” (Stergiou-Kita et al (2014a), p.16). Participants in Kosny et al’s study (2012) described being harassed at work by co-workers who believed them to be “milking the system” (p.443) while negative stereotypes led returning workers in two studies to actively restrict social contact with their co-workers. Participants in Choi et al’s study (2014) sought to avoid the rumours that were often spread about returning workers who were perceived as “malingerers” (p.4).
I was really self-conscious. ‘What do other people talk about in whispers when they see me doing exercise in the gym?’ […] So I did exercise alone and secretly”. (p.4)
Furthermore another study (Lysaght and Larmour-Trode 2008) reported that when co-workers trusted the injured worker and believed their claims to be true, they were more likely to provide support. One worker reported feeling he could rely on his co-workers to provide support as he felt they trusted him.
People here know me quite well and know that I work hard and I’m reliable and I don’t abuse the system, so when I’m injured, I’m injured, despite whether the injury is ‘invisible’ or not. (p.263)
Factors related to the culture of the workplace
Supportiveness of workplace culture
Several studies discussed the culture of the work environment in terms of how social support was facilitated. A participant in one study (Dunstan and Maceachen 2013) discussed the difference in her willingness to support colleagues in a supportive compared to a non-supportive workplace. She felt responsible to ‘pitch in’ in the former workplace whereas in the latter workplace she did not feel the need to help;
Quite frankly, I didn’t really care about the person with issues […] I came, I filled in my hours, I got paid, and I left. … The toxic environment didn’t lead to good relationships. (p.48)
Similarly, participants in another study (Kosny et al 2012) felt that the competitive culture of the electrical sector, where worries about job security were rife, and workers were divided into segregated teams, hindered the provision of social support. One co-worker reported ‘They want us to out-work one another’ (p.443). In this environment, helping another colleague would put one’s own job security at risk and therefore was not feasible; co-workers needed to prioritise their own well-being and job security before considering others.
Individualistic versus collectivistic workplace cultures
In addition to these findings that the individualistic priorities of workers in the electrical sector precluded social support, two studies discussed individualistic vs collectivistic workplace cultures, although with contrasting findings. Participants in one study (Dunstan and Maceachen 2013) reported feeling happier to put in extra work or allocate the lighter tasks to a returning worker if they felt their work group had a collective identity while participants in Tjulin et al’s (2011a) study who worked within a collectivistic culture were keen to simply replace the injured worker rather than provide special work accommodations for them. Another study (Tjulin et al 2011b) found that within workplaces where the workload was seen to belong to the worker, there was less tension in the workplace and workers were keen for their colleague to return to his own workload and reduce the stress on them.
Factors related to the quality of the organisation of the RTW plan
Quality of formal communication
One factor that appears to underlie several others in the provision of social support is the quality of formal communication within the workplace. In several studies, the lack of sufficient communication about the returning worker’s condition, limitations, and entitlements led to the proliferation of rumours, gossip, and misunderstandings, which hindered the provision of social support. The lack of social support was not necessarily malicious; a lack of formal information led to participants feeling ‘unequipped to give the support that was needed’ in Dunstan and Maceachen’s study (2013; p. 49) while participants in another study provided inappropriate support when they lacked understanding of the workers’ condition. In accordance, Tjulin et al (2011a) found that implicit communication about a worker’s return caused anxiety to be felt regarding how to act around the returning worker while a participant in Stergiou-Kita et al’s study (2014b) reported receiving “extensive support from coworkers who were educated by management about precautions to take to ensure effective wound healing” (p.503). However, contrary to the majority of studies included in this review, Stergiou-Kita et al (2014a) found that reduced communication concerning the returning worker’s condition prevented harassment and exclusion;
We have a strict privacy [policy]. Nobody else will know who is on a claim other than the immediate supervisor. Because in construction when you’re dealing [with] a predominantly male environment, he’ll [the worker will] be labelled, excuse my language, the dog f*****. He’ll be harassed. He will be ostracized by his co-workers (p.16).
Lack of understanding of RTW plans
A lack of understanding of the RTW process or of the co-worker’s role in the RTW process was often cited as a reason that social support had been inhibited. For example, co-workers who were unsure of the returning worker’s entitlements in line with the RTW scheme made health service workers returning from sickness absence in one study feel as if they were an aggravation if they attempted to attend medical appointments (Sager and James 2005).
Participants in two studies reported feeling social support may have increased if co-workers were more involved in planning the RTW process. They would then be aware of the rights of the returning worker, would be allowed input as to how they managed any additional work load, and could identify how best to support their colleague. However, co-workers interviewed in another study held quite different ideas about their involvement in planning the return; co-workers did not feel they should be involved in the process and stated they would rather be left to manage their own workload.
Allocation of work load
A common theme among eight of the studies was that the provision of modified work to a returning worker could incur resentment from co-workers, particularly if it was seen to be easy, or a duty reserved for more superior employees, in which case workers were believed to be receiving special treatment. Participants in Kosny et al’s study (2012) reported ‘sensing contempt from co-workers who felt they were now doing ‘cushy’ work’ (p.445).
Resentment also occurred if co-workers were expected to do extra work in order that the returning worker could receive accommodations. Participants in two studies saw this as a particular problem if the returning worker continued to be paid the same amount for doing less work.
Synthesis of findings
The factors discussed in this meta-ethnography combine to form a line of argument synthesis whereby the findings of the studies complement one another in order to generate new understanding, as defined by Noblit and Hare (1988). Many factors seem to interact with one another to influence the provision of social support. Furthermore, as in the model proposed by Dunstan and MacEachen (2014), it appears that the relationship between identified factors and social support may be mediated by the co-workers’ judgement of fairness of work accommodations. Although this concept of fairness was not specifically discussed in any of the studies it does seem to dominate many of the participants’ quotes and the primary authors’ interpretations.
Judgements of a lack of fairness made by co-workers have been observed to lead to restriction of support in a number of cases in the selected studies, for example:
- Where co-workers were not allowed input into the allocation of work tasks.
- Where co-workers believed they were being asked to do too much extra work.
- Where co-workers perceived the returning worker to be receiving special treatment.
Judgements of fairness might lead to provision of social support when these antecedent factors are reversed e.g. co-workers are allowed input into allocation of work tasks. One quote that demonstrates the importance of judgements of fairness is taken from Dunstan and Maceachen’s study (2013):
It’s going to cause resentment, like when they […] can only perform fifty percent of their tasks and they’re still getting paid. (p.50)
This participant predicts that resentment will occur when the amount of work performed by the returning worker and the amount of pay they receive, are not in proportion. This unfair situation is expected to lead to a restriction of social support.
It therefore appears that situational and dispositional factors within the RTW process may often be subject to a judgement of fairness in determining whether those factors will result in the provision of social support.
Discussion and Implications
Nature of Synthesis
Many factors have been identified in this review as contributing to the provision of social support or lack thereof, and generally the studies are in agreement regarding these factors i.e. they present as reciprocal translations. On three occasions there was a conflict between studies in their findings – with regard to whether individualistic or collectivistic workplace cultures best facilitate support, whether co-worker input in the RTW plans facilitates social support, and whether reduced communication about the worker’s communication hinders support or impedes bullying. These disagreements may be related to contextual differences between studies such as the nature of the work tasks or the culture of the country in which the workplace was located. For example, participants in Stergiou-Kita et al’s study (2014) who reported that limitations on communication reduced the harassment of returning workers, acknowledged that this was due to the workplace being male-dominated and hostile. In this setting, formal communication regarding the returning worker’s illness may not have reaped the same benefits as in more supportive workplace cultures. It is important, in taking the findings of this review forward, to recognise that measures taken to improve social support in one workplace may not be successful in another. Many of the included studies provided little information regarding the workplaces in which their participants worked and it would be valuable for future research to clearly document this in order that comparisons can be made between workplace contexts.
A line of argument was developed as a result of the synthesis of studies whereby the primary factors identified within the studies appear to both directly influence provision of social support and to indirectly influence it via the co-worker’s judgement of the fairness of work accommodations.
Factors that influence social support provision
This review draws together similar findings across a number of contexts regarding the factors affecting co-worker social support. Four over-arching categories of antecedent factors were found to consistently affect the provision of co-worker support in varied workplaces and cultures and this consistency of findings allows for greater confidence to be placed in the resulting recommendations for policy and development of theory.
The studies included in this review were mixed with regard to whether they investigated social support that was perceived by the returning worker or social support that co-workers reported providing. However remarkably similar factors were reported by both returning workers and co-workers. The one exception to this was that returning workers appeared to discuss negative stereotypes held about them more frequently than their co-workers reported them. This may have been due to co-workers being affected by a social desirability bias whereby they choose not to report undesirable, stereotypical beliefs to the researchers (as discussed by Krumpal, 2011), or it may be that in the state that returning workers in two studies described as ‘paranoid’ (Kirsh et al 2010, Sager and James 2005), stereotypical views present in broader societal discourse (e.g the media) were perceived where they were not existent in the specific workplace, reflecting the concept of internalised stigma (Brohan et al 2010).
Perceptions of fairness as a mediator
The line of argument developed through the process of meta-ethnography has found an increased body of evidence which broadly substantiates the model proposed by Dunstan and MacEachen (2014) in suggesting that co-workers’ judgements of fairness mediate the relationship between factors in the RTW process and support behaviours.
Fairness in the workplace is more commonly referred to in organisational research as organisational justice (Greenberg and Colquitt 2013). Further, perceptions of organisational justice have been found by Messer and White (2006) to positively affect organisational citizenship behaviours (OCBs). These are actions performed by employees that go beyond their job description for the benefit of either the organisation itself or for individuals within the organisation including co-workers e.g. re-arranging one’s work hours to allow another colleague to take annual leave. While OCBs performed for the benefit of co-workers have not directly been described as social support, there do seem to be a number of similarities in their definitions and thus Messer and White’s research (2006) further supports the line of argument that judgements of fairness affect social support provision.
Implications for practice and policy
There are a broad range of situations discussed in this review in which a perception of unfair work accommodations may be made and consequently lead to the restriction of social support. From these examples, it is possible to make some suggestions as to how co-workers’ perceptions of fairness may be changed. Of key importance to many instances in which unfairness was perceived, was a lack of understanding of the RTW plans, and of the returning worker’s condition. It appears essential therefore that formal communication is improved in the workplace; communication of the RTW plans ought to be explicit rather than spread through rumours which restrict the provision of appropriate social support (Dunstan and MacEachen 2013), and include a focus on encouraging support and tackling negative stereotypes. Co-workers can be included in the discussion of elements of RTW plans in order that they have a say regarding any extra work they are required to take on.
Although it may be reasonable to recommend supervisors improve formal communication regarding RTW plans, it is the employee’s right to decide whether to disclose information about their health to their employer and co-workers (Equality Act; Great Britain 2010). Furthermore it is unclear whether concealing or revealing a health problem, particularly a stigmatizing one, is more conducive to social support (Dunstan and MacEachen 2013, Kirsh et al 2012).
An additional recommendation would be to ensure supervisors are aware of the importance of their role both in promoting clear communication and also in modelling supportive behaviours. This may support the cultivation of a workplace culture in which social support is the norm and is fairly exchanged in times of need. As the supervisor appears to have such an influential role in developing a culture of support it may be fruitful for future reviews to seek to synthesise understanding of the factors affecting social support provided by supervisors in the RTW process.
The findings of this review and recommendations developed on their basis may additionally influence the work of practitioners in England and Wales’ new Fit for Work Service (Department for Work and Pensions, 2015) which the College of Occupational Therapists (2014) has identified as an emerging area in which occupational therapists may gain employment. The Service will allow companies and GPs to refer employees who have been absent due to sickness for an occupational health assessment in which a RTW plan will be developed so that both employee and employer can receive the support they need. The current review emphasises the need for employers to improve communication within the workplace, encourage co-worker support and include co-workers in RTW planning. Occupational therapists in work-support positions will have an important role in advising employers to adopt such changes.
The findings of this review also reinforce the importance of anti-stigma mental health campaigns and those that aim to improve awareness of mental health problems such as the UK’s Department of Health funded Time to Change campaign (Henderson et al 2012) as a lack of understanding of mental health conditions was a key factor identified as restricting the provision of social support within the workplace.
Limitations
All studies were appraised to be of either medium or good quality. However there was an absence in many studies of a consideration of the researcher’s assumptions, or relationship with the research. Reflexivity is of great importance when conducting qualitative research, particularly within a constructivist paradigm, as it allows the reader to fully appreciate how the interpretations presented have been constructed (Gough 2003). This lack of reflexivity may reduce the credibility of the initial authors’ interpretations on which this review is based and highlights the need for more reflexivity in this field of qualitative research.
An additional limitation is that most of the studies included in the review discussed social support as a one-dimensional concept yet many academics adopt House’s notion of a multifaceted social support (House 1981) comprising at least four different types of support. Accordingly the use of the blanket term social support in the selected studies could be seen as a weakness of this review, as the findings lack specificity and the rich detail that could be gained through the division of social support into its component parts. Future research would benefit from specifying the particular types of support that are affected by factors in the RTW process.
Conclusion
This review offers a detailed and extensive account of the factors consistently found to affect social support in the RTW process of individuals who have been absent due to sickness. These factors can be categorised into those relating to individual workplace actors, the condition, the culture of the workplace, and the quality of the organisation of the RTW plan. The review also offers new understanding regarding the association between perceptions of organisational justice and social support behaviours. A line of argument synthesis was used to demonstrate that the factors identified affect social support both directly and indirectly via the co-workers’ judgement of the fairness of work accommodations. Occupational therapists and other professionals involved in RTW planning could enhance the social support provided by co-workers, and consequently the success of an employee’s return by addressing the factors that may lead to a judgement of unfair work accommodations.
Yvette Wagner, MSc Health through Occupation; and Dr. Josh Cameron, Principal Lecturer in Occupational Therapy
References
Articles selected for inclusion in review
Baril R, Clarke J, Friesen M, Stock S, Cole D, the Work Ready group (2003) Management of return-to-work programs for workers with musculoskeletal disorders: a qualitative study in three Canadian Provinces. Social Science and Medicine, 57, 2101-2114.
Choi M, Kim H-R, Lee J, Lee H-E, Byun J, Won JU (2014) Workers’ experiences with compensated sick leave due to musculoskeletal disorder: a qualitative study. Annals of Occupational and Environmental Medicine [online], 26(33). Available at: http://link.springer.com/article/10.1186%2Fs40557-014-0033-0#page-1 Accessed on: 10.01.15.
Corbiere M, Renard M, St-Arnaud L, Coutu M-F, Negrini A, Sauve G, Lecomte T (2014) Union Perceptions of factors related to the return to work of employees with depression. Journal of Occupational Rehabilitation [online]. Available at: http://link.springer.com/article/10.1007%2Fs10926-014-9542-5 Accessed on: 10.01.15.
Dunstan DA, MacEachen E (2013) Bearing the brunt: co-workers’ experiences of work reintegration processes. Journal of Occupational Rehabilitation, 23(1), 44-54.
Kirsh B, Slack T, King CA (2012) The nature and impact of stigma towards injured workers. Journal of Occupational Rehabilitation, 22, 143-154.
Kosny A, Lifshen M, Pugliese D, Majesky G, Kramer D, Steenstra I, Soklaridis S, Carrasco C (2012) Buddies in Bad Times? The Role of Co-workers After a Work-Related Injury. Journal of Occupational Rehabilitation, 23(3), 438-449.
Lysaght RM, Larmour-Trode S (2008) An exploration of social support as a factor in the return-to-work process. Work, 30(3), 255-266.
Mansfield E, Stergiou-Kita M, Kirsh B, Colantonio A (2014) After the storm: The social relations of return to work following electrical injury. Qualitative Health Research, 24(9), 1183-1197.
Nordqvist C, Holmqvist C, Alexanderson K (2003) Views of laypersons on the role employers play in return to work when sick-listed. Journal of Occupational Rehabilitation, 13(1), 11-20.
Norlund S, Fjellman-Wiklund A, Nordin M, Stenlund T, Ahlgren C (2013) Personal resources and support when regaining the ability to work: an interview study with exhaustion disorder patients. Journal of Occupational Rehabilitation, 23(2), 270-279.
Sager L, James C (2005) Injured workers’ perspectives of their rehabilitation process under the New South Wales workers compensation system. Australian Occupational Therapy Journal, 52, 127-135.
Stergiou-Kita M, Mansfield E, Dalter L, Colantonio A (2014a) Good Intentions? Employer representative conceptualizations and, challenges to the workplace accommodation process: The case of electrical injuries. Employee Responsibilities and Rights Journal [online]. Available at: http://link.springer.com/article/10.1007%2Fs10672-014-9242-5#page-1 Accessed on: 10.01.15.
Stergiou-Kita M, Mansfield E, Bayley M, Cassidy JD, Colantonio A, Gomez M, Jechke M, Kirsh B, Kristman V, Moody J, Vartanian O (2014b) Returning to work after electrical injuries: workers’ perspectives and advice to others. Journal of Burn Care and Research, 35(6), 498-507.
Tjulin A, MacEachen E, Edvardsson Stiwne, Ekberg K (2011a) The social interaction of return to work explored from co-workers experiences. Disability and Rehabilitation, 33(21-22), 1979-1989.
Tjulin A, MacEachen E, Ekberg K (2010) Exploring workplace actors experiences of the social organization of return-to-work. Journal of Occupational Rehabilitation, 20(3), 311-321.
Tjulin A, MacEachen E, Ekberg K (2011b) Exploring the meaning of early contact in return-to-work from workplace actors’ perspective. Disability and rehabilitation, 33(2), 137-145.
Other references
Bisiker J, Millinchip K (2007) Developing a work rehabilitation project: ‘Equal pathways to work’. British Journal of Occupational Therapy, 70(6), 259-263.
Black DC, Frost D (2011) Health at work – an independent review of sickness absence. Norwich: The Stationary Office.
Brohan E, Elgie R, Sartorius N and Thornicroft G (2010) Self-stigma, empowerment and perceived discrimination among people with schizophrenia in 14 European countries: the GAMIAN-Europe study. Schizophrenia Research, 122(1-3), 232-238.
Brouwer S, Reneman MF, Bultmann U, van der Klink JJ, Groothoff JW (2010). A prospective study of return to work across health conditions: perceived work attitude, self-efficacy and perceived social support. Journal of Occupational Rehabilitation, 20(1), 104-112.
Cesario S, Morin K, Santa-Donato A (2002) Evaluating the level of evidence of qualitative research. Journal of Obstetric, Gynecologic and Neonatal Nursing, 31(6), 708-714.College of Occupational Therapists (2014) Health and Work Service heralds new job opportunities for OTs. Available at: https://www.cot.co.uk/news/health-and-work-service-heralds-new-job-opportunities-ots Accessed on: 27.07.14.
Coole C, Drummond A, Watson P, Worthington E, Hammond A (2013) Supporting workers with musculoskeletal conditions: a survey of United Kingdom occupational therapists’ communications with patients and their employers. British Journal of Occupational Therapy, 76(11), 478–486.Critical Appraisal Skills Programme (2013) Qualitative Research Checklist. Available at: http://media.wix.com/ugd/dded87_951541699e9edc71ce66c13bac4734c69.pdf Accessed on: 26.07.14.
Department for Work and Pensions (2015) Fit for Work: guidance for employers. Available at: https://www.gov.uk/government/publications/fit-for-work-guidance-for-employers Accessed on: 27.05.15.Dunstan DA, MacEachen E (2014) A Theoretical Model of Co-worker Responses to Work Reintegration Processes. Journal of Occupational Rehabilitation, 24(2), 189-198.
Eakin J, MacEachen E, Clarke J (2003) ‘Playing it smart’ with return to work: Small workplace experience under Ontario’s policy of self-reliance and early return. Policy and Practice in Health and Safety, 1(2), 20-41.
Gough B (2003) Deconstructing reflexivity. In: Finlay L and Gough B, eds. Reflexivity: A practical guide for researchers in health and social sciences. Oxford: Blackwell Science Ltd. 2003. 21–35
Great Britain. Parliament (2010) Equality Act 2010. London: The Stationery Office.
Greenberg J, Colquitt JA (2013) Handbook of Organizational Justice. Oxford: Psychology Press.
Henderson C, Corker E, Lewis-Holmes E, Hamilton A, Flach C, Rose D et al (2012) England’s Time to Change Antistigma Campaign: One-Year Outcomes of Service User-Rated Experiences of Discrimination. Psychiatric Services, 63(5), 451-457
House JS (1981) Work, stress and social support. Reading, MA: Addison-Wesley.
Inman J, McGurk E, Chadwick J (2007) Is Vocational Rehabilitation a Transition to Recovery? British Journal of Occupational Therapy, 70(2), 60-66.Messer BAE, White FA (2006) Employees’ mood, perceptions of fairness, and organizational citizenship behaviour. Journal of Business and Psychology, 21(1), 65-82.
Noblit GW, Hare RD (1988) Meta-Ethnography: Synthesizing Qualitative Studies. London: Sage publications. Paterson BL, Thorne SE, Canam C, Jillings C (2001) Meta-Study of Qualitative Health Research. London: SAGE Publications.Waddell G, Burton AK (2006) Is work good for your health and well-being? London: The Stationary Office.